Introduction
Pharmaceutical manufacturers leave little room for error. Maintaining drug stability, preventing contamination, and satisfying FDA, EMA, and global regulatory requirements all depend on getting material selection right.
A single defective component can trigger batch rejections, product recalls, and regulatory citations that cost millions.
Borosilicate glass is widely referenced across pharmaceutical operations, yet many producers underestimate what it actually delivers: fewer contamination incidents, higher sterilization pass rates, smoother regulatory submissions, and preserved drug efficacy from fill line to patient administration.
This article explains the practical advantages borosilicate glass delivers across pharmaceutical manufacturing, the operational risks of choosing inferior alternatives, and how to maximize value through proper specification and system integration.
Key Takeaways
- Type I borosilicate glass meets the highest standards per USP <660>, EP 3.2.1, and JP classifications for hydrolytic resistance
- Prevents container-closure interaction by not leaching ions into pharmaceutical products—critical for injectables and biologics
- Withstands autoclave sterilization (121°C) and depyrogenation (250°C+) without cracking or structural failure
- Using lower-grade glass increases batch contamination risk, product recalls, and FDA enforcement actions
- Borosilicate sight glasses and process components must meet the same compliance standards as primary packaging in GMP-regulated environments
What Is Borosilicate Glass?
Borosilicate glass is a specialized formulation composed primarily of silica (approximately 75-80%) and boron trioxide (10-13%), engineered for high chemical inertness and strong thermal resilience. These properties make it the preferred material for pharmaceutical operations where drug integrity and process reliability are critical.
The global pharmacopeial system classifies pharmaceutical glass into three distinct types based on hydrolytic resistance—the ability to resist chemical interaction with aqueous solutions:
Glass Classification by Hydrolytic Resistance:
- Type I (Borosilicate): Highest hydrolytic resistance due to chemical composition; suitable for all parenteral products
- Type II (Treated Soda-Lime): Surface-treated glass with high resistance; suitable for most acidic and neutral aqueous parenterals
- Type III (Soda-Lime): Moderate resistance from base glass composition; typically not used for parenteral products
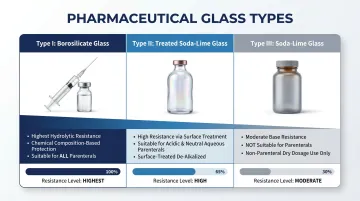
According to USP <660> standards, Type I borosilicate must meet stringent limits: maximum 0.1 mL of 0.02 M HCl per gram of glass in the Glass Grains Test, compared to 0.85 mL for Type II/III. This tenfold difference in alkali content directly translates to superior protection against chemical leaching during drug storage.
That chemical resistance is what drives its use across drug storage, sterile manufacturing, and regulatory-critical packaging applications throughout a product's lifecycle.
Key Advantages of Borosilicate Glass in Pharmaceutical Operations
Pharmaceutical quality teams measure performance in concrete terms: contamination incident rates, batch rejection frequency, sterilization efficiency, stability study results, and regulatory audit findings. Each advantage below maps directly to those metrics.
Superior Chemical Resistance
Borosilicate glass exhibits very low reactivity with pharmaceutical compounds. Unlike soda-lime glass, it does not leach alkali ions or exchange chemicals with drug products—even under prolonged storage or exposure to aggressive formulations.
How This Works in Practice:
When filled with injectable solutions, biologics, or highly sensitive APIs, Type I borosilicate containers maintain the drug's original pH, concentration, and molecular integrity throughout shelf life. The glass composition creates an inert barrier that prevents container-closure interaction, the degradation process where packaging materials chemically react with drug substances.
Measurable Operational Value:
Container-closure interaction can alter drug pH, degrade active ingredients, and introduce particulates that force recalls. In October 2024, Staska Pharmaceuticals recalled Ascorbic Acid Solution for Injection due to glass particulates in vials — FDA cited risks including local irritation, vascular blockage, and potential stroke or death. In July 2019, Fresenius Kabi recalled Fluorouracil Injection after glass particulates appeared in retained samples.
A single contamination event triggers compounding costs: complete batch rejection, FDA Form 483 observations, market withdrawals, and reputational damage that far exceeds any savings from choosing lower-grade glass.
KPIs Directly Impacted:
- Batch rejection rate
- Product contamination incidents
- Stability study pass rate
- Drug recall frequency
- Regulatory audit citations
When Chemical Resistance Matters Most:
- Parenteral products (IV drugs, injectables, biologics) that bypass the body's natural defenses
- Highly acidic or alkaline formulations that accelerate ion leaching
- Long shelf-life products where slow ion migration accumulates to harmful levels
Thermal Stability and Sterilization Compatibility
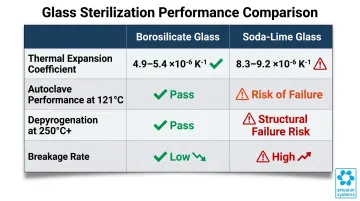
Borosilicate glass possesses a coefficient of thermal expansion (CTE) of approximately 4.9-5.4 × 10⁻⁶ K⁻¹, roughly one-third that of soda-lime glass (8.3-9.2 × 10⁻⁶ K⁻¹). This low CTE means borosilicate expands and contracts minimally under rapid temperature changes, a baseline requirement for pharmaceutical sterilization.
Real-World Application:
Pharmaceutical manufacturers rely on two primary sterilization methods:
- Autoclave sterilization: 121°C moist heat for 15-20 minutes
- Depyrogenation: 250°C dry heat for 30 minutes minimum per USP <85>, USP <797>, and USP <1228.1> standards
Borosilicate glass survives both processes without cracking or micro-fracture formation. Soda-lime glass, with its higher thermal expansion coefficient, risks structural failure under identical conditions.
The Cost of Breakage:
Glass breakage during sterilization introduces particulate contamination into sterile products and causes fill-line downtime. According to a 2018 PDA Letter analysis, approximately 20 billion vials are processed annually for injectable drugs globally, yet only 6 recalls related to cracks and breakage were announced over a six-year period for borosilicate containers, demonstrating the material's reliability under production conditions.
Rescheduling sterilization batches, replacing damaged containers, and validating line cleanliness after breakage events compound production costs and delay time-to-market for new drug launches.
KPIs Directly Impacted:
- Sterilization cycle pass rate
- Fill-line downtime hours
- Glass breakage rate during processing
- Production cycle time
- Sterility assurance level (SAL) compliance
When Thermal Stability Matters Most:
- High-volume sterile manufacturing operations
- Biologics requiring cold-chain storage plus terminal sterilization
- Any process where containers move rapidly between temperature extremes
Regulatory Compliance and USP Type I Classification
Type I borosilicate glass is the only glass grade universally accepted by USP <660>, EP 3.2.1, and JP standards for parenteral pharmaceutical packaging without requiring additional surface treatment. This baseline advantage over Type II and Type III glass simplifies the entire product development pathway.
How This Translates Operationally:
Selecting Type I borosilicate from initial development reduces the scope of required extractables/leachables studies, accelerates stability protocol design, and positions manufacturers favorably during FDA pre-approval inspections and NDA/BLA reviews. FDA guidance issued in July 2024 specifies that changes to glass container types require Prior Approval Supplements (PAS), extensive validation, and both accelerated and real-time stability data.
Measurable Operational Value:
Using non-compliant glass for parenteral products can result in FDA Form 483 observations, warning letters, or import alerts. In May 2025, FDA issued Warning Letter WL#699291 to Staska Pharmaceuticals citing glass particulate contamination, inadequate investigation of batch failures, and CGMP violations under 21 CFR 211.192, 211.100(a), and 211.113(b). These enforcement actions halt production, block product distribution, and require costly remediation before operations can resume.
KPIs Directly Impacted:
- Regulatory submission approval timeline
- FDA/EMA audit observation frequency
- Drug stability study pass rate
- Time-to-market for new products
- Cost of compliance remediation activities
When Regulatory Compliance Advantages Matter Most:
- Launching new injectable or parenteral products
- Operations under active FDA or EMA oversight
- Companies scaling from clinical trial to commercial manufacturing
What Happens When the Wrong Glass Is Used
Selecting the wrong glass type doesn't just create a quality problem — it creates a compliance problem. Type II and Type III glass containers introduce three categories of failure that can compromise drug integrity, trigger regulatory action, and surface months after the original sourcing decision.
Ion Leaching and pH Shift
Lower-grade glass releases alkali ions — sodium and calcium — into drug solutions, altering pH and degrading active pharmaceutical ingredients. This process accelerates with acidic or alkaline formulations and worsens over long-term storage.
Glass Delamination
In 2011, the FDA issued an advisory on glass delamination — the formation of thin glass flakes (lamellae) that detach from container inner surfaces and enter drug solutions. Multiple recalls in 2010 and 2011 followed, prompting industry-wide surveillance programs and the development of Chemical Durability Ratio (CDR) testing as an early warning method.
Thermal Failure During Sterilization
Glass lacking adequate thermal resistance cracks during autoclaving or depyrogenation. Each crack introduces particulate contamination and triggers fill-line shutdowns for investigation.
Downstream Operational Consequences:
- Batch rejections discovered during quality control testing
- Forced product recalls after market distribution
- FDA Form 483 observations and warning letters
- Fill-line production shutdowns for investigation and remediation
- Costly re-validation if packaging must be changed post-approval

What makes these failures particularly costly is their delayed discovery. Many go undetected until ICH Q1A(R2) stability studies or post-market surveillance flag a problem. By that point, the financial and regulatory consequences of the original sourcing decision may be years in the making.
How to Get the Most Value from Borosilicate Glass Components
Borosilicate glass delivers full operational value only when three conditions are met:
Correct Specification
Select the appropriate Type I grade and container format — vials, ampoules, or sight glasses — based on drug formulation, fill volume, and process requirements. Verify supplier documentation confirms compliance with USP <660>, EP 3.2.1, and JP standards before finalizing any component.
Validated Sourcing
Work with suppliers who provide complete regulatory documentation. Key requirements include:
- Material certifications with lot-specific traceability
- Extractables/leachables data relevant to your drug formulation
- Batch-specific test results from qualified laboratories
- FDA 21CFR177.2600 compliance and ISO9001 quality system certification
Artesian Systems manufactures tri-clamp borosilicate sight glasses (1.5" to 6" sizes) with FDA 21CFR177.2600 compliance and ISO9001 certification — built to withstand -40°C to 500°C and pressures up to 150 PSI, including autoclave sterilization and depyrogenation cycles.
Proper System Integration
Integrate borosilicate components into sanitary process systems with appropriate passivation, filtration integrity testing, and CIP (clean-in-place) compatibility. Material selection and system design should be treated as a single engineering decision, not two separate procurement steps.
Ongoing Performance Validation
Review outcomes against measurable benchmarks:
- Contamination incident rates per 100,000 units produced
- Sterilization cycle pass rates (target: >99.5%)
- Stability study failure rates
- Regulatory audit observation frequency
Revisit material and system choices whenever formulations change, production volumes scale, or new regulatory guidance is issued. Component selection is a living engineering decision — one that evolves with your process.
Conclusion
Borosilicate glass is a performance-critical component whose chemical inertness, thermal durability, and regulatory acceptance protect drug safety, manufacturing efficiency, and compliance outcomes. Those advantages grow stronger when the correct Type I grade is consistently specified, properly integrated into validated sanitary systems, and matched to the product and process at hand.
Choosing lower-grade alternatives carries costs that go well beyond material savings. The downstream consequences include:
- Batch rejections and lost production time
- Product recalls and FDA enforcement actions
- Compromised patient safety
- Reputational damage that takes years to recover from
Treat borosilicate glass selection as a strategic engineering decision—revisit it alongside formulation changes, scale-up milestones, and regulatory updates. In pharmaceutical manufacturing, material performance determines operational outcomes, and getting that specification right from the start is far less costly than correcting it after the fact.
Frequently Asked Questions
Is borosilicate glass used in the pharmaceutical industry?
Yes, Type I borosilicate glass is the industry standard for pharmaceutical packaging, particularly for parenteral products. USP <660>, EP 3.2.1, and JP classifications designate it as the highest hydrolytic resistance grade, suitable for all injectable drugs, biologics, and sensitive formulations where chemical interaction between container and drug must be eliminated.
Which is better: Pyrex or borosilicate?
Pyrex laboratory glassware is manufactured from borosilicate glass, so the comparison is between different borosilicate formulations. However, pharmaceutical-grade Type I borosilicate glass meets stricter USP <660> hydrolytic resistance standards than standard Pyrex labware, making it the required choice for drug packaging applications.
Why is Type I borosilicate glass required for injectable drugs?
Because injectables bypass skin and digestive defenses entirely, leached ions or particulates from packaging enter the bloodstream directly. USP and EP mandate Type I borosilicate for parenterals because its chemical inertness prevents container-closure interaction that could compromise drug efficacy or harm patients.
What is glass delamination and why does it matter in pharmaceuticals?
Delamination is the formation of thin glass flakes (lamellae) that separate from the inner container surface and enter drug solutions. FDA's 2011 advisory identified this as a contamination risk that can cause product recalls and potential patient harm through particulate injection into the bloodstream.
Can borosilicate glass withstand autoclave sterilization?
Yes. Borosilicate glass's low thermal expansion coefficient (4.9–5.4 × 10⁻⁶ K⁻¹) allows it to withstand autoclave sterilization at 121°C and depyrogenation at 250°C+ without cracking — meeting sterile manufacturing requirements without structural compromise.
What is the difference between Type I, Type II, and Type III pharmaceutical glass?
The three types differ by hydrolytic resistance:
- Type I (borosilicate) — highest resistance by composition; required for all parenterals
- Type II (surface-treated soda-lime) — suitable for most acidic or neutral aqueous solutions
- Type III (untreated soda-lime) — moderate resistance; limited to solid dosage forms and non-parenteral use